Evaluation and monitoring
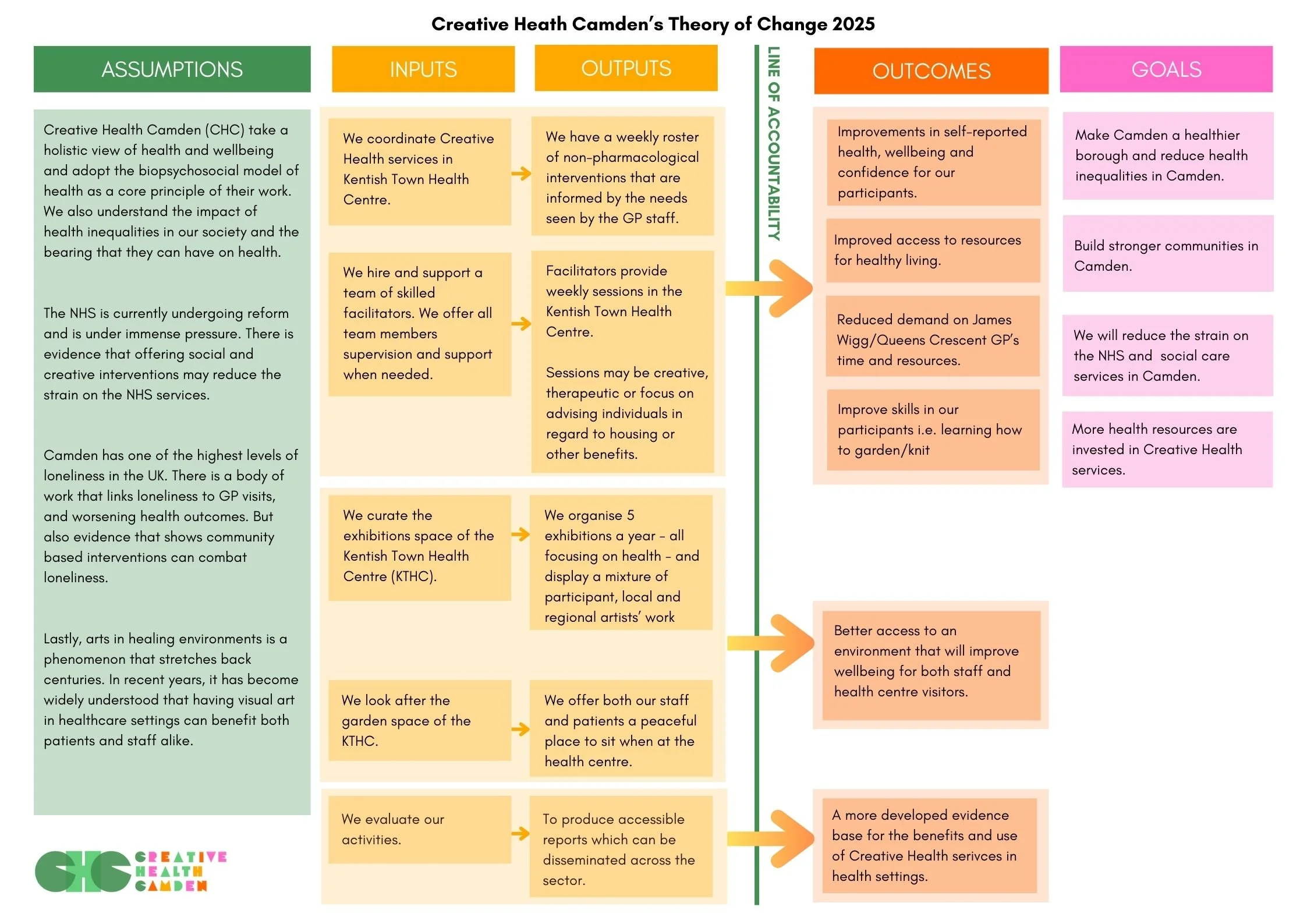
One of the priorities for CHC for 2025 was solidifying our evaluation and monitoring processes. Part of this was developing our Theory of Change. This sets out our intentions as a charity and gives us something to evaluate our programmes against.
Please see below for our Theory of Change, as of 4th December 2025.
We have also considered our approach to evaluation and monitoring:
CHC is charity that works at the intersection of arts and health. When we do monitoring and evaluation we conduct it to improve our services and further our knowledge of the impact that we are having.
Core Principles:
Accessibility:
This refers to both how we conduct our research and how we disseminate it. We aim to use inclusive language and avoid the use of highly academic terms, we also aim to use the participants first language (if possible), and design evaluation methods that are inclusive to any disabilities or health conditions that our participants may have (i.e. using a BSL interpreter with deaf participants).
Non-hierarchal:
Whilst there is a Programme and Evaluation Lead at CHC who will oversee monitoring and evaluation work, all will aim to be codesigned with facilitators and participants. This means that the Programme and Evaluation Lead may ask prompting questions, but the way participants chose to answer it will be usually up to them (i.e. using drawings or words)
Iterative:
We will constantly review and update our procedures. We are always learning and evolving to be of the highest standard we can be. This means we encourage you to constantly review this guidance as we update it.
Ethical:
CHC will take direction from the National Arts in Hospital Network (NAHN) Evaluation Guidance regarding ethics. The main principles are:
Informed Consent
We will ensure that participants are able to understand and give full consent. All data that we will collect will be explained in detail to the participant, this may include Special Category Data, information regarding self-reported health, and potentially medical information. All data will be stored according to our privacy policy.
To gain full consent we may use simple language or a translator. We also understand that literacy levels differ between patients, these situations will be considered on a case-by-case basis and trustees may be consulted when necessary. For example, recorded voice note giving consent may be deemed appropriate for patients who struggle with literacy
Maintain Confidentiality and Anonymity
All information will be kept confidential, and no one will be identifiable.
Store Data Safely
All data will be stored according to our privacy policy.
Ensure Safety and manage risk
We will be sensitive and considerate of participants needs
Support will be offered if needed
All safeguarding policies will be adhered to.
We will anticipate and plan for any negative impacts that our work may have on our participants.
Avoid bias
Impartiality will be paramount.
Honesty will be valued and data will be collected in a way that allows for all opinions to be valued and heard.
Reciprocal and non-extractive process
Only data that is needed for an evaluation will be collected
We aim to make data collection engaging and to not take away from the joy of our sessions.
We aim to make it non-imposing on the participants.
Dissemination:
A digital written version of our reports will always be on our website, and so they will exist in the public domain, as well as be used internally for reviews and funding forms.
We believe that anyone who is involved in evaluation and monitoring should be able to understand the final reports. This means that we may disseminate our research in a variety of ways and mediums. For example, using a translator to read out a report in Sylheti for our Bengali population, or using visual images to tell a story for those who struggle with reading. We may also create mini ‘zines’ with our research findings in, this is to ensure that there is an accessible format of our long-form reports.